Vaccination and Social Distancing
How can vaccine status and beliefs impact social distancing?
Author: Krishane Patel | 29/05/2024Summary
How strongly do people adhere to social distancing? In this
study I examine how vaccine statuses and belief in the effectiveness of
vaccines impact social distancing. The results show that belief strength
has differential effects for different vaccine statuses on social
distancing. For fully vaccinated indiviudals, vaccine belief was shown
to reduce social distancing, but partially and unvaccinated individuals
were shown to distance more as their beliefs grew. In addition, the
research shows a similar trend for vaccine intentions, as well as
egocentric mechanisms for judgements of others vaccination.
Read the full working paper here: Link
to article
Background
During the COVID-19 pandemic, governments worldwide implemented various
policies to
reduce transmission and protect health systems and vulnerable populations,
such as
the elderly and immunocompromised (Kadambari, Klenerman, & Pollard, 2020;
Mikolai,
Keenan, & Kulu, 2020; Rout, 2020). While specific measures varied, the core
strategy
was to delay the virus's impact until a vaccine could be rolled out on a
mass scale
(Kissler et al., 2020; Riel & Wit, 2020). Common preventive policies
included social
distancing and mask mandates, driven by evidence showing that new
information and
altered risk perceptions can change behavior (Gaube, Lermer, & Fischer,
2019; Wise
et al., 2020). Governments encouraged remote work, limited social
gatherings, and
mandated physical distancing, with some regions mandating mask usage earlier
than
others. For instance, mask use in the UK was mandated from June 2020 (Murphy
et al.,
2021), while countries like Austria and Indonesia enforced vaccine mandates
due to
issues with vaccine hesitancy (Soares et al., 2021).
Vaccines such as Pfizer-BioNTech, Oxford/AstraZeneca, and Moderna initially
showed
high efficacy in reducing the risk of COVID-19 infection and hospitalization
(Pilishvili et al., 2021; Sadoff et al., 2021; Voysey et al., 2021).
However, the
emergence of variants like Delta and Omicron reduced vaccine efficacy,
leading to
concerns about increased transmission even among vaccinated individuals
(Riemersma
et al., 2022; Buchan et al., 2022). As vaccine efficacy declined,
alternative public
health measures like social distancing and mask usage remained essential.
The
combination of these factors sometimes led to risk compensation, a
phenomenon where
individuals adjust their behavior based on perceived lower risks,
potentially
increasing overall risk (Peltzman, 1975; Underhill, 2013).
Risk compensation has been studied in various contexts, such as seatbelt
use, HIV
prevention, and contraception (Evans & Graham, 1991; Eaton & Kalichman,
2007;
Shukla, Pullabhotla, & Arends-Kuenning, 2021). In the context of COVID-19,
there is
mixed evidence regarding risk compensation behaviors. Some studies, such as
Luckman
et al. (2021), show that mask mandates led to reduced social distancing,
while other
research, like Buckell et al. (2021), found evidence of risk compensation
after
vaccination. However, the phenomenon is not universal, with some research
showing no
significant risk compensation, such as a study on Taiwanese healthcare
workers (Sun
et al., 2022). Theoretical frameworks, like the Social Amplification of Risk
Framework (Kasperson et al., 1988), help explain how risk perceptions are
shaped by
competing signals, which can lead to changes in behavior across different
contexts.
To investigate this hypothesis, an online natural experiment was ran
recruiting individuals from the United States to take part in a distance
preference task, evaluating population differences between vaccine status in
conjunction with demographic factors and strength of belief in the vaccine
as well as perceived risk.
Method
Sample
A total of 760 participants were recruited from Prolific (www.Prolific.co.uk) in July 2021, completing the experiment on the Qualtrics platform (www.Qualtrics.com). Participants were paid 0.70c to complete the experiment (at a rate of $8.40/hour).
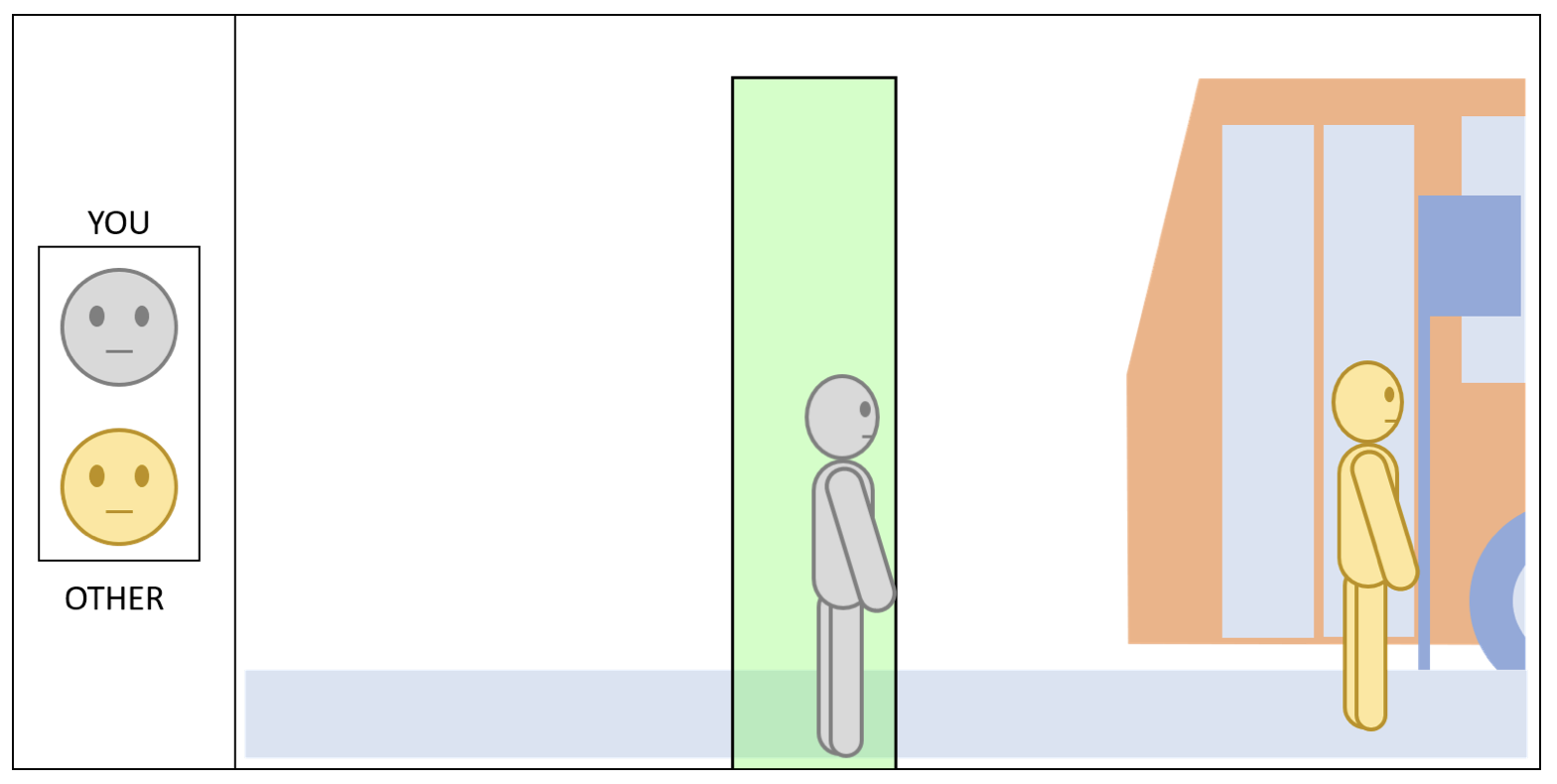
Participants placed an avatar of themselves to indicate the closest distance they would be willing to position themselves from another person (described as a stranger) in six different scenarios in a 2 (Inside or Outside) x 3 (Sitting, Standing or Walking) factorial design. There were 17 different locations they could place the avatar, which based on the scaling of the avatar and scene, denoted 0.25m intervals between 0m and 4m. After completing the distance preference task, participants were asked to answer a short survey to understand more about participants (demographic) as well as their vaccine status, and beliefs about the vaccines and COVID-19 virus. Ethical approval for this study was granted by the University of Warwick’s Decision Research at Warwick committee (HSSREC: 75/20-21).
Analysis
A fixed effects model was used to analyse the data regressing vaccine status and vaccine belief (and their interaction) along with a vector of control variables on social distance judgements. Analysis was conducted using R with the afex package. Data is available on the OSF website .
Results
Vaccine Status and Belief on Social Distancing Behavior
My research reveals that belief in the COVID-19 vaccine has a differential
effect on
social distancing, depending on an individual’s vaccination status. For
fully
vaccinated individuals, stronger belief in the vaccine was associated with a
reduction in social distancing. Conversely, partially vaccinated and
unvaccinated
individuals exhibited increased distancing as their belief in the vaccine's
efficacy
grew. These differing responses suggest important behavioural implications,
particularly at the extremes of belief. See below in
Figure 2.
The contrast in social distancing behaviour between vaccinated and
unvaccinated
individuals becomes more evident when examined side by side. Pairwise
comparisons
between the groups uncovered significant differences.
For instance, fully vaccinated individuals with weaker beliefs in the
vaccine
maintained a greater physical distance from others, standing approximately
2.15
metres away. On the other hand, partially vaccinated individuals with
similarly weak
beliefs stood much closer, around 0.68 metres—indicating a noticeable
difference in
perceived risk or precautionary behaviour. Unvaccinated individuals with
weaker
vaccine beliefs fell in between, keeping a distance of approximately 1.11
metres.
However, when belief in the vaccine was strong, the pattern shifted. Fully
vaccinated individuals stood slightly closer, at about 1.89 metres.
Meanwhile, both
partially vaccinated and unvaccinated individuals increased their distancing
significantly, standing at 2.38 metres and 2.36 metres, respectively.
These results highlight the complex role vaccine beliefs play in shaping
social
behaviour, regardless of vaccination status. Fully vaccinated individuals
with high
confidence in the vaccine may feel a greater sense of security, which in
turn leads
them to reduce their social distancing. In contrast, partially vaccinated
and
unvaccinated individuals who strongly believe in the vaccine appear to take
additional precautions, likely due to a heightened awareness of their
incomplete or
absent protection.
In summary, it is not just vaccination status that determines social
distancing
behaviour; belief in the vaccine's effectiveness also plays a pivotal role.
This
suggests that public health strategies should address both vaccination
status and
belief systems to effectively guide behaviour and reduce the spread of
COVID-19.
Judgements on Vaccine Status Distribution
An interesting aspect of the study explored people’s perceptions of how
common
different vaccine statuses (fully vaccinated, partially vaccinated, or
unvaccinated)
are within the population. The analysis revealed that individuals tend to
overestimate the prevalence of their own vaccination status, a phenomenon
known as
egocentric bias.
For instance, fully vaccinated individuals estimated that 42.61% of the
population
was also fully vaccinated, significantly higher than the estimates provided
by
partially vaccinated individuals (34.57%) and unvaccinated individuals
(33.47%).
Unvaccinated individuals
displayed the same bias, estimating that 42.82% of the population was
unvaccinated,
while fully vaccinated and partially vaccinated individuals provided much
lower
estimates. A
similar pattern emerged among partially vaccinated participants, who
estimated a greater proportion of the population shared their status,
compared to
lower
estimates from the other groups.
This egocentric bias suggests that people tend to see their own vaccination
status as the norm, which could influence how different groups interpret
public
health messaging and campaigns.
Conclusion
This study highlights important population differences in social
distancing behavior associated with COVID-19 vaccination status and beliefs
in
vaccine efficacy. While not implying causation, the results suggest that
individuals' vaccination status and their beliefs about vaccine
effectiveness are
associated with distinct patterns of distancing behavior.
Among fully vaccinated individuals, stronger belief in the vaccine’s
effectiveness
correlates with reduced social distancing, potentially reflecting a sense of
security. In contrast, partially vaccinated and unvaccinated individuals
with strong
beliefs in vaccine efficacy tend to increase their distancing behaviors,
possibly
due to an awareness of incomplete or absent vaccination protection. These
patterns
highlight varying responses across groups, suggesting that vaccine beliefs
interact
with perceived risk in shaping behavior.
Additionally, the observed egocentric bias, where individuals tend to
overestimate
the prevalence of their own vaccination status, suggests that people may
interpret
public health messages through the lens of their perceived majority status.
This
could influence how different groups respond to public health efforts.
In summary, these findings underscore the importance of addressing both
vaccination
status and belief systems in public health strategies. By acknowledging
these
population differences, health campaigns may better engage diverse groups
and
promote effective social distancing practices, supporting efforts to
mitigate
COVID-19 transmission in varied demographic contexts.
What is the impact for public health policy?
- Risk behaviours are influenced by interventions and people's belief in these interventions. While fully vaccinated individuals tend to distance less as their belief in the vaccine increases, partially vaccinated and unvaccinated individuals distance more with stronger beliefs.
- Egocentric bias affects perceptions of vaccination distribution. People tend to overestimate the prevalence of their own vaccine status, potentially shaping their views of public health efforts and policies.
- Egocentric Bias Skews Public Perception. Different groups may have different risk perceptions based on egocentric mechanisms and behave differently.
- Public Health Messaging May Be Perceived Differently. Different groups might interpret public health messages in ways that align with their own perceived majority status, leading to impaired effectiveness of public health campaigns.
- Tailored Communication Strategies Are Crucial. Public health campaigns may need to be more tailored to specific groups to counteract these egocentric biases.
Conclusion
This study underscores the complex relationship between vaccine beliefs, vaccination status, and social distancing behaviors. The findings reveal that stronger belief in vaccine efficacy leads to varied behavioral responses:
- Fully vaccinated individuals tend to reduce social distancing as their confidence in vaccine efficacy grows, possibly reflecting a sense of security.
- Partially vaccinated and unvaccinated individuals increase social distancing with stronger vaccine beliefs, likely compensating for their perceived incomplete or absent protection.
Additionally, the study highlights an egocentric bias: individuals consistently overestimate the prevalence of their own vaccination status within the population. This bias could influence how people interpret public health messaging and respond to campaigns.
Implications for Public Health Policy
The findings emphasize the need for tailored communication strategies that account for these behavioral differences. Public health messaging should clarify that vaccination complements, rather than replaces, social distancing measures. Such clarity can mitigate the potential for risk compensation, particularly in the face of highly transmissible variants like Delta and Omicron.
Future Directions
Further research is needed to validate these findings in real-world settings and explore interventions that balance public confidence in vaccines with adherence to other protective behaviors, like social distancing. By addressing these nuances, public health campaigns can better navigate the complex dynamics of behavior during pandemics, ultimately enhancing compliance and reducing transmission.
References
- Buchan, S. A., Chung, H., Brown, K. A., Austin, P. C., Fell, D. B., Gubbay, J. B., ... & Kwong, J. C. (2022). Effectiveness of COVID-19 vaccines against Omicron or Delta infection. medRxiv. https://doi.org/10.1101/2021.12.30.21268565
- Eaton, L. A., & Kalichman, S. C. (2007). Risk compensation in HIV prevention: Implications for vaccines, microbicides, and other biomedical HIV prevention technologies. Current HIV/AIDS Reports, 4(4), 165-172. https://doi.org/10.1007/s11904-007-0024-7
- Evans, L., & Graham, J. D. (1991). Risk reduction or risk compensation? The case of mandatory safety-belt use laws. Risk Analysis, 11(1), 9-16. https://doi.org/10.1111/j.1539-6924.1991.tb00600.x
- Gaube, S., Lermer, E., & Fischer, P. (2019). The concept of risk perception in health-related behavior theory and behavior change. In M. S. Wogalter (Ed.), Handbook of Warnings (pp. 1-10). CRC Press.
- Kadambari, S., Klenerman, P., & Pollard, A. J. (2020). Why the elderly appear to be more severely affected by COVID-19: The potential role of immunosenescence and CMV. Reviews in Medical Virology, 30(5), e2144. https://doi.org/10.1002/rmv.2144
- Kasperson, R. E., Renn, O., Slovic, P., Brown, H. S., Emel, J., Goble, R., ... & Ratick, S. (1988). The social amplification of risk: A conceptual framework. Risk Analysis, 8(2), 177-187. https://doi.org/10.1111/j.1539-6924.1988.tb01168.x
- Kissler, S. M., Tedijanto, C., Goldstein, E., Grad, Y. H., & Lipsitch, M. (2020). Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science, 368(6493), 860-868. https://doi.org/10.1126/science.abb5793
- Luckman, A., Zeitoun, H., Mourad, R., & Plonsky, O. (2021). Risk compensation during COVID-19: The impact of face mask usage on social distancing. PLOS ONE, 16(6), e0253871. https://doi.org/10.1371/journal.pone.0253871
- Mikolai, J., Keenan, K., & Kulu, H. (2020). Intersecting household-level health and socio-economic vulnerabilities and the COVID-19 crisis: An analysis from the UK. Sociological Research Online, 25(4), 1-17. https://doi.org/10.1177/1360780420962866
- Murphy, J., Vallières, F., Bentall, R. P., Shevlin, M., McBride, O., Hartman, T. K., ... & Hyland, P. (2021). Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nature Communications, 12(1), 29. https://doi.org/10.1038/s41467-020-20226-9
- Peltzman, S. (1975). The effects of automobile safety regulation. Journal of Political Economy, 83(4), 677-725. https://doi.org/10.1086/260352
- Pilishvili, T., Fleming-Dutra, K. E., Farrar, J. L., Gierke, R., Mohr, N. M., Talan, D. A., ... & Schrag, S. J. (2021). Interim estimates of vaccine effectiveness of Pfizer-BioNTech and Moderna COVID-19 vaccines among health care personnel—33 U.S. sites, January–March 2021. Morbidity and Mortality Weekly Report, 70(20), 753-758. https://doi.org/10.15585/mmwr.mm7020e2
- Riemersma, K. K., Grogan, B. E., Kita-Yarbro, A., Halfmann, P. J., Segaloff, H. E., Kocharian, A., ... & O'Connor, D. H. (2022). Shedding of infectious SARS-CoV-2 despite vaccination. medRxiv. https://doi.org/10.1101/2021.07.31.21261387
- Rout, A. (2020). COVID-19 and the elderly: A review of the evidence on risk factors, clinical features, diagnosis and management. British Journal of Community Nursing, 25(9), 438-444. https://doi.org/10.12968/bjcn.2020.25.9.438
- Sadoff, J., Gray, G., Vandebosch, A., Cárdenas, V., Shukarev, G., Grinsztejn, B., ... & Schuitemaker, H. (2021). Safety and efficacy of single-dose Ad26.COV2.S vaccine against COVID-19. New England Journal of Medicine, 384(23), 2187-2201. https://doi.org/10.1056/NEJMoa2101544
- Shukla, A., Pullabhotla, H., & Arends-Kuenning, M. (2021). Risk compensation and contraceptive use among women in Sub-Saharan Africa. Studies in Family Planning, 52(2), 159-176. https://doi.org/10.1111/sifp.12155
- Soares, P., Rocha, J. V., Moniz, M., Gama, A., Laires, P. A., Pedro, A. R., ... & Nunes, C. (2021). Factors associated with COVID-19 vaccine hesitancy. Vaccines, 9(3), 300.